



Buy-in
An upside of our current longevity movement is how hyperaware we now are about the benefits of exercise. Few other interventions within our control can offer such a positive dramatic impact on lifespan and healthspan. 1
A downside, however, is injury — something my Substack brother Paul von Zielbauer of Aging With Strength and I both know all too well. So we tackled the topic in our video above.
Getting hurt after 50 is often a result of one of two scenarios:
People who’ve been exercising or athletic most of their lives. Now the body parts are beat up and can’t sustain the load or regimen they used to. But the mind still says: “Let’s do this!” (That’s Paul.)
People new to movement who are excited about data showing it’s not too late for exercise to improve health and longevity at any age. They jump in eagerly but go too hard, too fast without a proper ramp-up period. (That’s me.)
Here’s a primer on what injuries are most common, why, and strategies to tweak your routine to avoid them. In the Cash-out section, you’ll find links to related past articles on this topic.
Post
Why are older adults more prone to injury when exercising?
Injuries often occur when the demand of the activity exceeds the current capacity of the tissue, balance system, or recovery system.
Recovery slows with age. Injured athletes age 45 and older recover about 15% to 18% more slowly than someone who is 30, according to data Paul cites in our episode. Our skin thins, making it more susceptible to cuts and lacerations. And bone density declines, making us more prone to fractures.2
So what are common drivers of exercise-related injuries? Some examples:
Returning too fast to exercise after inactivity.
Adding too much weight too quickly.
Skipping balance and mobility work.
Doing high-repetition activities without recovery.
Underestimating fall risk in activities that seem “easy.” (Think, pickleball or dog-walking. More on that in a moment.)
What are common injuries after age 50?
I took ten studies examining exercise injuries among adults age 50 and older, why they occur, frequency and the most common injuries.
Then I asked the latest paid model of ChatGPT to summarize the findings into a simple chart.
Note: These injuries should not be viewed as a conclusive list — but rather as a general indicator of where risk might occur in common activities.
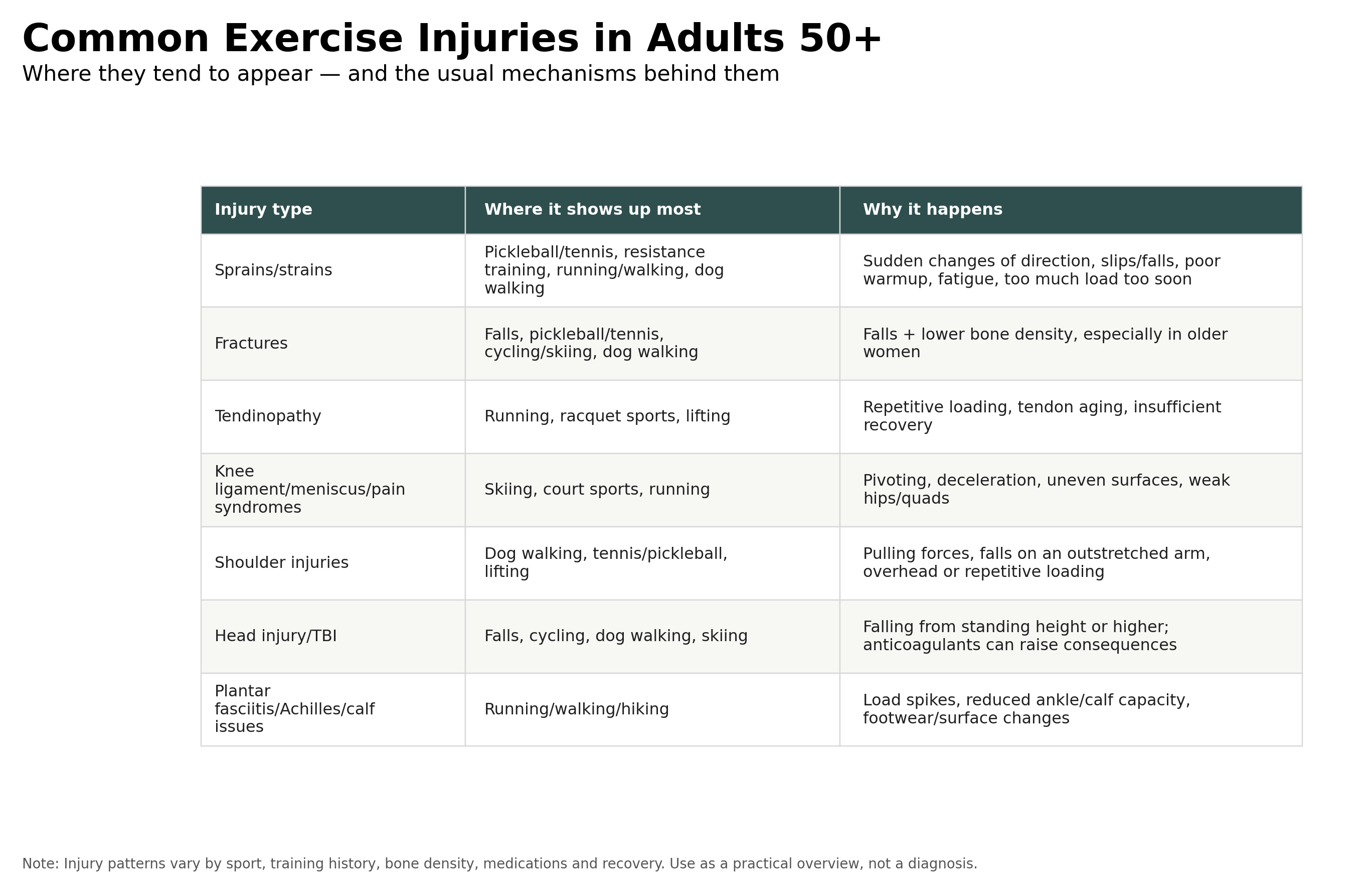
In one study included in the mix, golf (22.8%), pickleball (17.0%), tennis (13.4%), and weight lifting (12.9%) accounted for most injuries in people 55 and older.
The most common injuries for these sports were fracture (pickleball and tennis) and sprain/strain (golf and weight lifting).3
*Bonus: If you listen to our conversation above, you’ll get to hear Paul’s rant about pickleball.
What strategies may help mitigate injury?
When I first got serious about getting in shape in my mid-40s, I did a lot of things wrong. Got excited about a new sport — obstacle course racing — and then rushed into training. Lifted too much weight, too soon. Increased my running mileage without building slowly. Overused body parts like my forearms and shoulders in my excitement to get better at things like swinging from rings and monkey bars.
The result: forearm tendonitis, plantar fasciitis, ankle sprains, partial hamstring tears. Oh, and a nasty rope burn from learning to climb a rope barefoot. (That one is just plain dumb.)
My governing principle now is to treat my body like a book of matches — and do everything possible to keep anything from igniting by practicing the prevention techniques below.
If I feel a niggle or pain coming on, like a match got struck, I’m doing everything I can to put out that flame before it turns into a bigger fire. That means reducing my workout load, and strategically deploying ice, heat, rest and physical therapy (I’ve got two great PT practitioners as part of my medical pit crew.)
Here’s what my prevention strategy looks like:
1. Includes balance + functional movement training
For adults 50+, this is probably the single most important injury-prevention principle. As you age into your 60s and beyond, fall-related injuries become a major driver of fractures, head injuries, sprains, and shoulder/wrist trauma.
You want to become “stumble proof.”
Strategy: At least 2–3 days a week, I include squats or sit-to-stands, step-ups, calf raises, single-leg balance, lateral stepping and backward walking — otherwise known as “retro walking.” (See link in Cash-out).
A great exercise I recently added: Stand on one leg and toss a tennis ball back and forth between your hands for 30 seconds. Harder than it sounds.
2. A more diversified exercise diet
Over the past decade, I’ve gotten really good at carrying heavy things and running for a long time in the mountains. There are benefits to this, no doubt. But I now think of it as being a bit “dumb strong” because I ignored form, my core, and tiny little muscles you never think of.
Now I’m including yoga, pilates and taking classes such as “Better Backs and Balance” in addition to carrying 40 lb. buckets and sandbags. It’s early days, but I can feel a difference.
Strategy: Don’t be a one-note workout wonder. If you love strength, make sure you get cardio and vice versa. Include activities that make you move in different directions (yes Paul, like pickleball) strengthen your core, protect your back and tend to your feet. More details in the Cash-out section below.
3. Train consistently — but progress gradually
As I mentioned above, I blew this one when I first began training for obstacle course training. Shot out of the gate too hard and fast and paid for it.
For older adults, the mistake is often not strength training itself; it is too much intensity, too much novelty, or poor progression.
Strategy:
Don’t go wild with strength training in the beginning — 1-2 days of modest training is a good way to ease in.
Use exercises you can perform with clean technique.
Leave 1–3 reps “in reserve” instead of training to failure (i.e. — you can’t lift the weight anymore.)
Increase one variable at a time: weight, reps, sets, speed, range of motion, or frequency.
For tips on avoiding running injuries, see link in the Cash-out section to an interview with my former coach, Olympian Jessica O’Connell.
4. Always warm up — and include some dynamic movement
A warmup should prepare the nervous system, joints, tendons, and muscles for the activity you are about to do.
I prefer including dynamic movements versus static stretching alone.
Strategy: A simple 5-10 minute routine is generally sufficient. Here are two solid options:
A basic routine that checks a lot of boxes from the National Academy of Sports Medicine.
A slightly more advanced one I like from Michael Easter over at the Two Percent Substack.
Cash-out
To dig deeper on injury prevention, here’s a compilation of past “Not Too Late” articles on the topic: (Note: content older than 12 months is for paying subscribers.)
Step up: How to keep our feet & ankles strong. And why. (Link)
How to avoid running injuries and ease back into running — 8 tips from an Olympian. (Link)
Why ‘retro walking’ might be worth adding to your daily routine. (Link)
You probably don’t have enough muscle to age well. Here’s how to change that. (Link)
Fighting the ‘midlife assassin.’ Do you move like an old person moves? Or like a younger one does? (Link)
Heeding the ‘niggle’ and why it can protect you from injury (Link)
As always, find something you love. Dig in. Stick with it when things get hard. And double down on the basics.
Wendy
About me:
I’m Gwendolyn Bounds — an author, speaker and journalist. Currently, I work at The Wall Street Journal Leadership Institute as the Senior Vice President & Head of Content. My latest book is “Not Too Late: Break the Cycle of Sameness and Reimagine Your Limits.”

Disclaimer: Any work or ideas expressed in this forum are mine alone and do not represent my employer, The Wall Street Journal. I do not receive payment for products and services mentioned in my newsletter.
Sources & deeper exploration:
Arem, Hannah, Steven C. Moore, Alpa Patel, et al. “Leisure Time Physical Activity and Mortality: A Detailed Pooled Analysis of the Dose-Response Relationship.” JAMA Internal Medicine 175, no. 6 (2015): 959–967. (Link)

